Featured
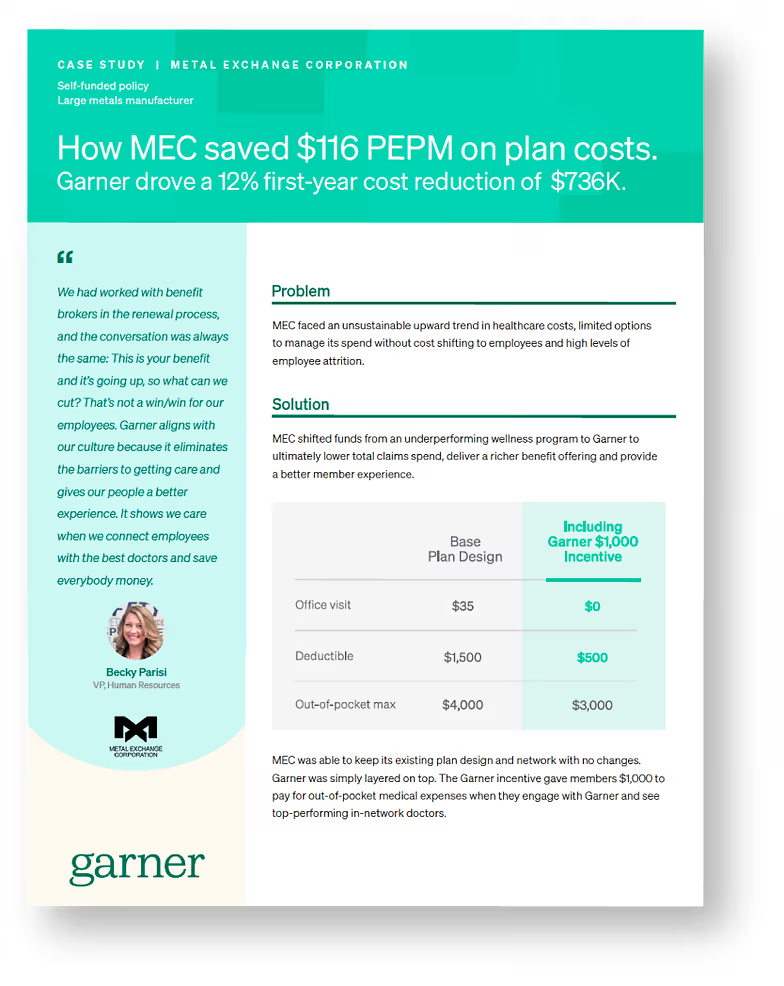
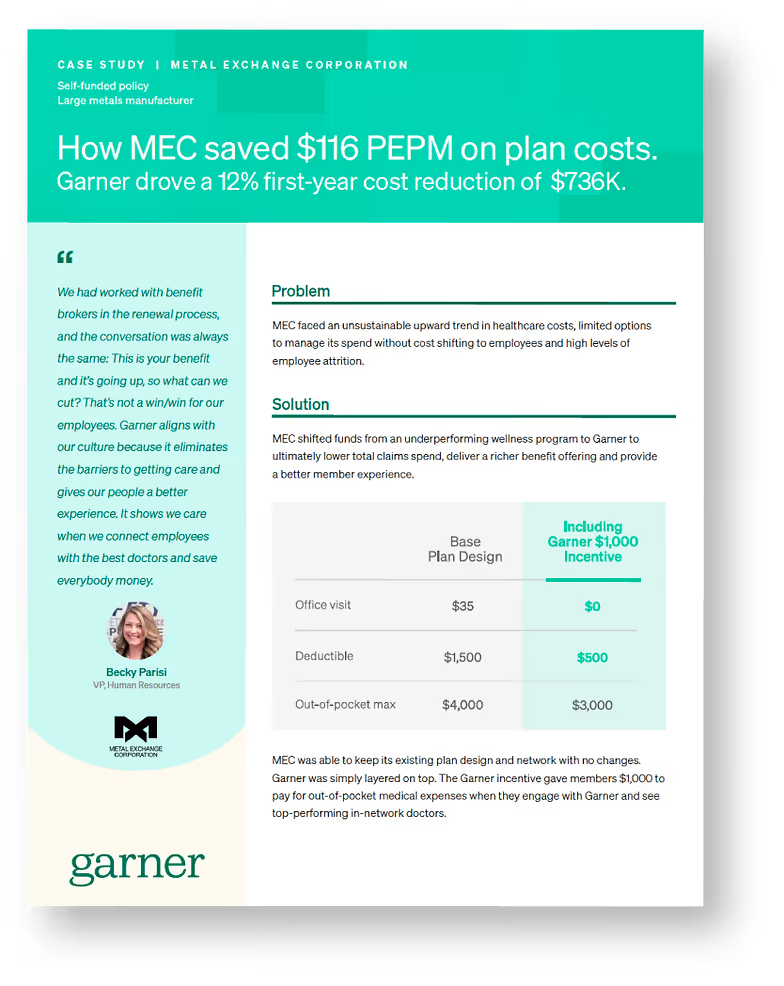
How a large metals manufacturer saved $116 PEPM on plan costs and drove a 12% first-year cost reduction of $736K.
“Garner aligns with our culture because it eliminates the barriers to getting care and gives our people a better experience. It shows we care when we connect employees with the best doctors and save everybody money.”